
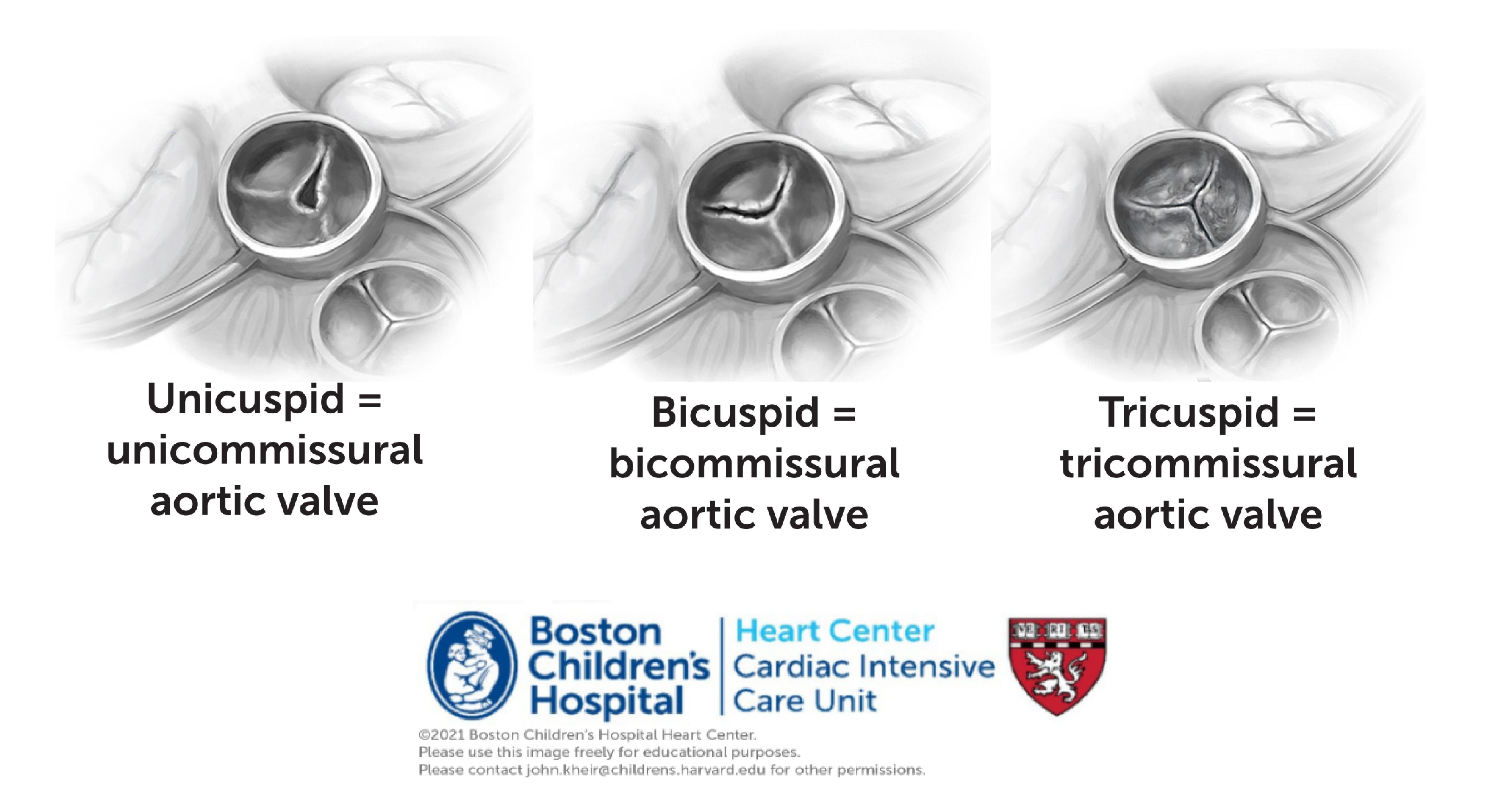
Anatomy. Critical AS may occur as a native disease or following in utero BD in the setting of HLHS. The AV morphology varies between unicuspid and tricuspid. In addition to AV stenosis and regurgitation, the pathology associated with poor LV flow-through impairs development of the LV, MV complex, frequently causing LA HTN and its sequelae. The LV may not be apex forming and the MV papillary muscles may be displaced towards the base, limiting leaflet mobility and causing MS or MR.
Physiology. The clinical definition of ‘critical’ AS is that the circulation fails when PGE are discontinued. Signs of circulatory failure may include signs of LA HTN (pulmonary edema), significant right to left ductal shunting (post-ductal desaturation [until complete PDA closure], respiratory acidosis from dead space ventilation), as well as poor pulses, gray skin color, decreased UOP and metabolic acidosis. In many cases, the LA is hypertensive (e.g. ASD gradient is elevated), but lung compliance may be spared and CXR may be clear if the RA pressure is low due to robust lymphatic compensation. In these cases, congested peribronchial lymphatics may compress the airways and cause wheezing.
Intervention. When the LV and MV appear to be of sufficient size to support the circulation (i.e. not HLHS/MS/AS, a distinction that requires some judgement), the initial intervention may be BD of the AV. This may relieve stenosis and stroke work while improving cardiac output, but may at times also cause aortic regurgitation.
Management. Following BD AV in the newborn with critical AS, the first step is assess the circulation following ductal closure, assessing the circulation as above. How quickly to wean the ventilator depends upon the stability of the circulation, the degree of lung water, the degree of pulmonary hypertension, and any comorbidities. If the pulses are strong, the CXR is clear, and there is no metabolic acidosis, the patient may often be extubated within 24 hours. In other cases, there are sequelae of LA HTN or it is not clear that the circulation is adequate. There may be LV dysfunction, EFE, AR, or MS/MR which compromise forward flow and cause LA HTN. If for this reason, the patient is unable to wean from the ventilator, it is often beneficial to provide time on the ventilator for the LV to relax while providing diuresis and adequate nutrition (monitoring for chylous effusions). During this time is may be helpful to maintain lung recruitment using a high PEEP strategy.
If this pathway fails, it is common to repeat imaging and cardiac catheterization and to consider ways to decompress the LA and augment the circulation. As discussed on the following pages, options include a Ross operation (if the primary lesion is thought to be the AV) or S1P, in which case the LA is decompressed by atrial septectomy and the systemic circulation augmented by the RV. However, in some cases, the LV is quite EFE-bound and may impede RV filling due to adverse ventriculo-ventricular interactions.
Videos from the BCH Cardiac Registry
Aortic Arch Obstruction Lecture – Stephen Sanders, MD [PDF] [PPT with video]
Important articles
Pre-intervention morphologic and functional echo characteristics of neonates with critical left heart obstruction: a Congenital Heart Surgeons Society (CHSS) inception cohort study
A large multi-institutional study, describe the distribution of the functional and morphological spectrum in patients with critical left-sided heart disease; Slieker MG, et al.; Eur Heart J Cardiovasc Imaging 2019.
Fetal interventions for congenital heart disease
The discussion on the rationale, patient selection, technical aspects, and outcomes of percutaneous, ultrasound-guided fetal cardiac intervention for structural congenital heart disease; Freud LR, et al.; Curr Opin Pediatr 2016
Aortic Valve Interventions in Pediatric Patients
The summary pieces of evidence of AV interventions in pediatric patients; Bouhout, et al.; Semin Thorac Cardiovasc Surg 2019.
Hybrid approach as a bridge to BiV repair in critical AS
– Biventricular repair after the hybrid Norwood procedure
BiV repair after an initial hybrid Norwood approach; Sojak V, et al.; Eur J Cardiothorac Surg 2019