Interpreting a chest radiograph in the cardiac ICU (also known as chest X-ray, or CXR) can be challenging. Here are a few basics to help get you started.
Identification
By far the most common error in CXR interpretation. (The name and MRN have been removed here to preserve anonymity.)

Positioning of endotracheal tube
The ETT can be seen in the trachea by its two radiopaque lines. Sometimes the air in the cuff can be visualized. The ETT should terminate above the carina and below the thoracic inlet.
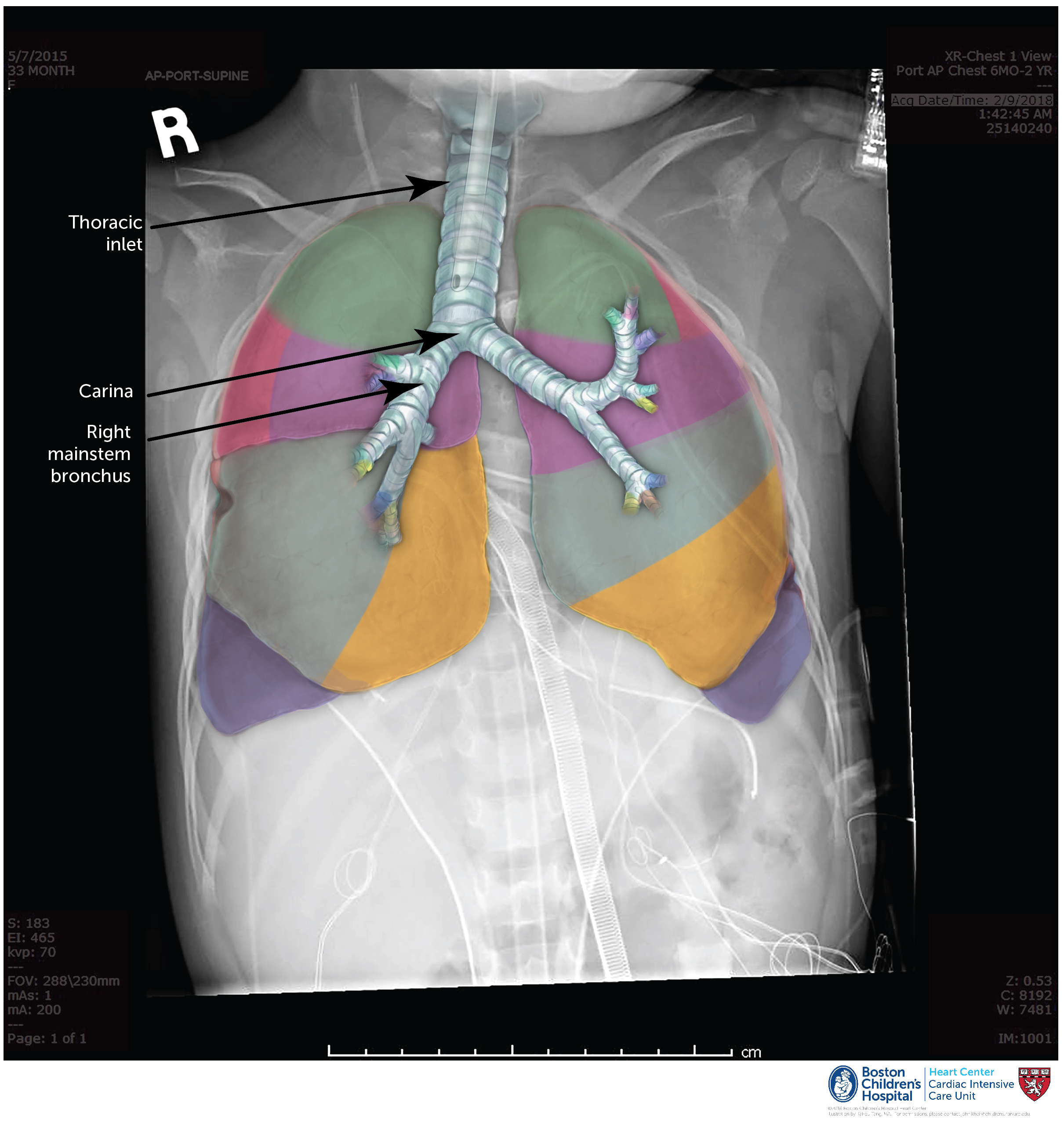 It is important that the ETT does not enter the right mainstem bronchus since the left lung may not then be ventilated. In neonates, placing a towel roll under the shoulders may suffice to move the ETT up 0.5 cm. Always remember, ‘the hose follows the nose’: extending the neck (as if looking up at the sky) moves the ETT up in the trachea, and flexing the neck (as if looking down to the ground) moves it down.
It is important that the ETT does not enter the right mainstem bronchus since the left lung may not then be ventilated. In neonates, placing a towel roll under the shoulders may suffice to move the ETT up 0.5 cm. Always remember, ‘the hose follows the nose’: extending the neck (as if looking up at the sky) moves the ETT up in the trachea, and flexing the neck (as if looking down to the ground) moves it down.
Positioning of chest drains
These may be in the right pleural cavity, the left pleural cavity, the pericardial cavity, or in the mediastinum. When the drain enters all of these cavities, it is colloquially referred to as an ‘around the world’ chest drain.

Positioning of vascular catheters
- The tip of an internal jugular catheter should be within the SVC or SVC-RA junction.
- Right atrial lines may be placed through the body of the RA (as shown) or more commonly through the right atrial appendage.
- Left atrial lines (not shown) may be placed through the left atrial appendage or more commonly through the right upper pulmonary vein (sometimes appearing as a backwards 7).
- Pulmonary artery catheters (not shown) may enter the right atrium and be fed antegrade into the MPA, or alternatively may be placed into the infundibulum or directly into the MPA using a tourniquet.

Positioning of temporary pacing wires
- Atrial pacing wires are sutured directly to the surface of the right atrium. By convention, atrial wires are always brought out to the right of the patient’s chest, even in the setting of dextrocardia.
- Ventricular pacing wires are sewn through the epicardial surface. By convention, ventricular wires are always brought out to the left of the patient’s chest, even in the setting of dextrocardia.

Positioning of enteric tubes
- Sump tubes should end in the stomach. Replogle tubes (in neonates) are typically single lumen. Salem sump tubes are dual lumen (the larger clear one for suction and the blue one for venting and equilibration of gastric pressure); in this case there is a small radiolucent space that should be placed no lower than the GE junction.
- Feeding tubes may be placed in the stomach, at the pylorus, or post-pyloric. In abdominal situs solitus (normal position of the abdominal viscera), the stomach sits to the left and the pylorus is just to the (patient’s) right of the spine. When there is question about feeding tune position, a lateral projection can be performed – the pylorus and duodenum hug the pancreas just anterior to the spine (i.e. very posterior in the abdomen).

Positioning of ECMO cannulae
The position of ECMO cannulae is critically important to maintaining perfusion of all vital organs. Central cannulation (shown here) is typically performed with a single venous cannula in the right atrium and a single arterial cannula in the transverse aorta. Alternatively, particularly in newborns following S1P, a ‘chimney graft’ may be left sewn onto the innominate artery and used to place the arterial cannula.
 When cannulation takes place via the carotid artery, the tip of the arterial cannula should be at the thoracic inlet and oriented towards the left chest. The arterial cannula should never be seen to be heading straight towards the heart; in these cases, the cannula tip may be in the ascending aorta, at the aortic valve, across the aortic valve, or within a BTS (see below) – all of which significantly compromise systemic perfusion and must be addressed immediately.
When cannulation takes place via the carotid artery, the tip of the arterial cannula should be at the thoracic inlet and oriented towards the left chest. The arterial cannula should never be seen to be heading straight towards the heart; in these cases, the cannula tip may be in the ascending aorta, at the aortic valve, across the aortic valve, or within a BTS (see below) – all of which significantly compromise systemic perfusion and must be addressed immediately. 
Echocardiography may be helpful in delineating the precise location of the instrumentation when there are questions.
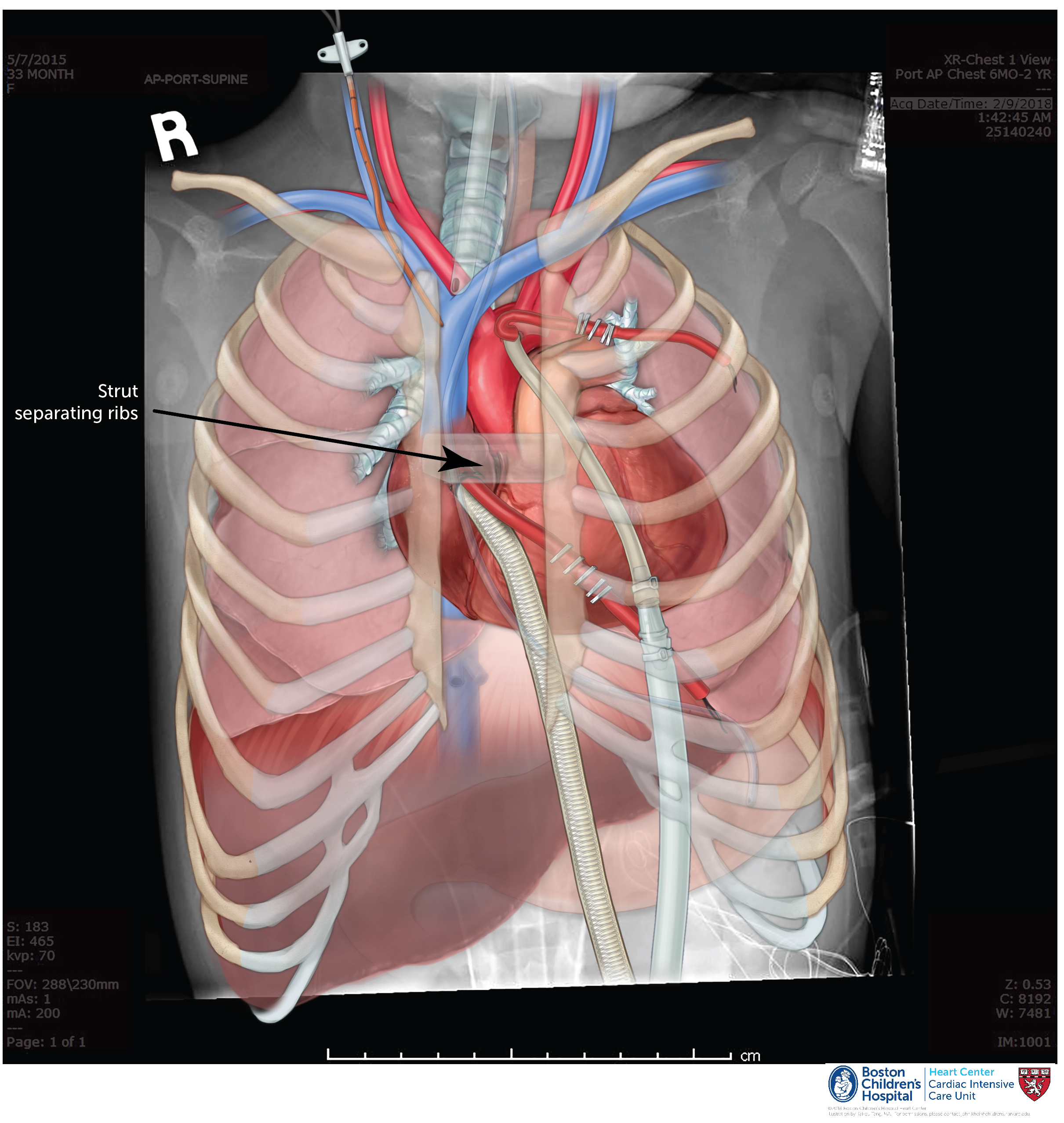
Strut
A strut is material used to stabilize the distance between the sternal edges. Often, a strut is placed to widen this distance, though it can also be used to bring the edges together as an iterative step in sternal closure. Struts can be made from chest tubes or cut-off syringes, and are typically 1-3 cm long. Not all open sterna have a strut in place.
Esmark
The Esmark dressing is a sterile elastic barrier that is sewn to the soft tissues around the sternal edge. This is covered by a final sterile iodine-containing dressing (called an Ioban) that adheres to the anterior chest wall.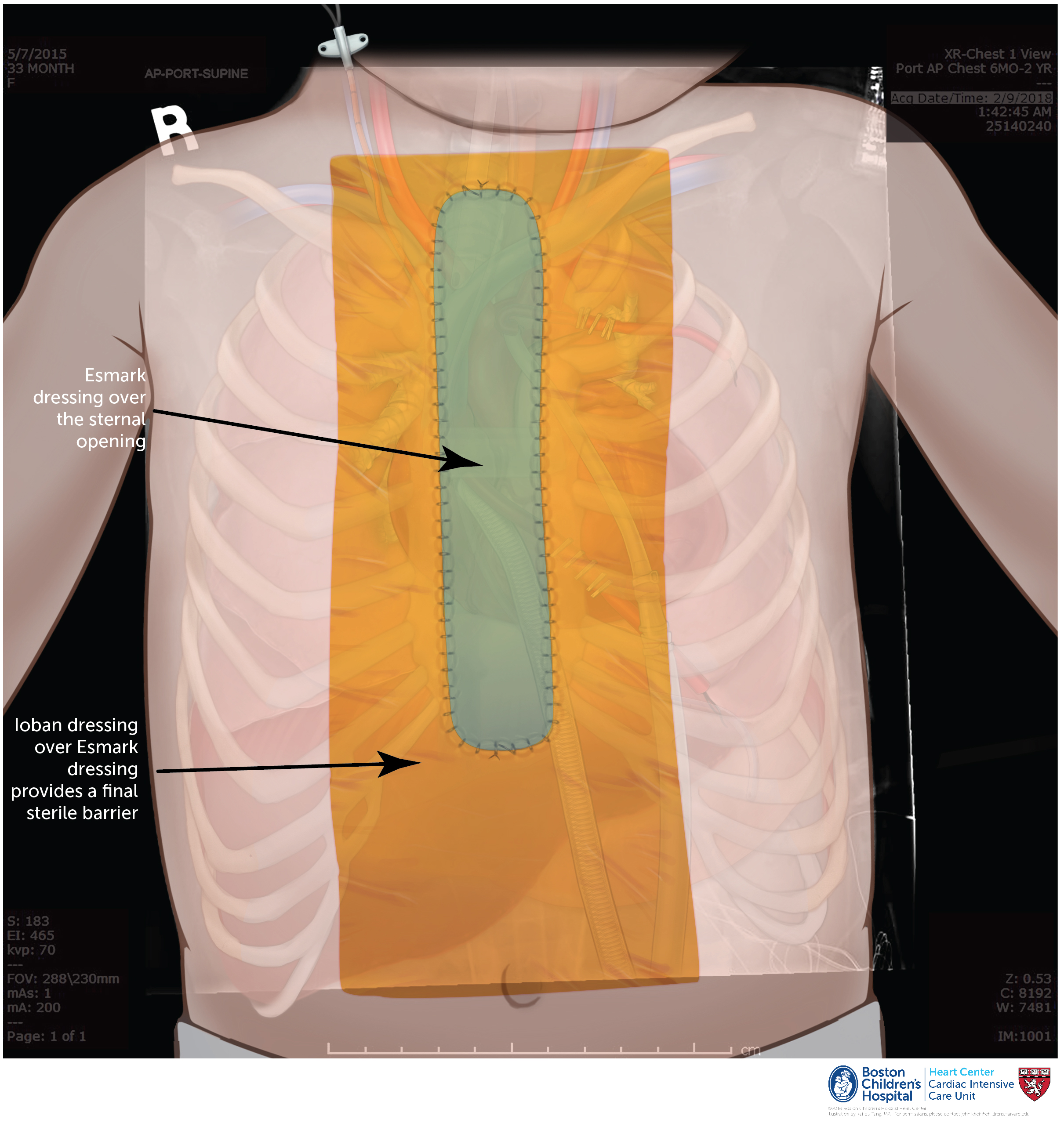
Revisions
July, 2018 – John Kheir, MD