Anatomy
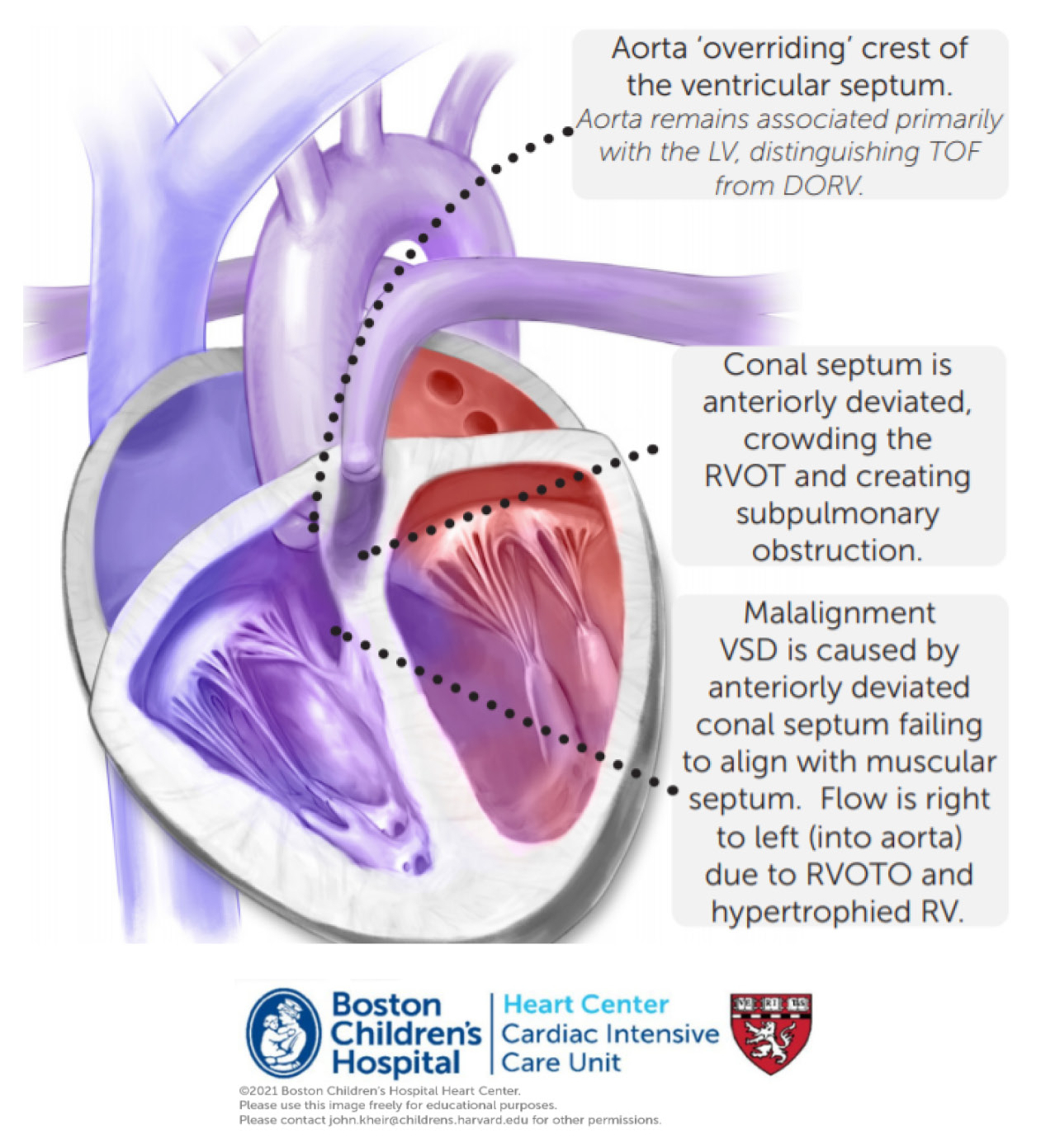
Tetralogy of Fallot exhibits four components, although they are all caused by unequal arterial septation and anterior deviation of conal septum.
- Subvalvar and commonly valvar pulmonary stenosis or atresia; 10-15% of patients exhibit a trileaflet pulmonary valve with near normal dimension
- Anterior malalignment VSD
- Overriding aorta
- Right ventricular hypertrophy
- May be associated with CAVC
Physiology
The clinical course of TOF/PS depends upon the degree of subvalvar muscular obstruction, PV hypoplasia and concomitant RVOTO. Patients with PV Z-score <3 and/or significant muscle bundles obstructing the RVOT are at increased risk for severe hypoxemia in the newborn period. Generally, if saturations are >80% following ductal closure, patients may be discharged until elective biventricular repair at 3-6 months of age. However, if a patient exhibits hypercyanotic spells or persistent desaturation in the newborn period our general approach has been neonatal repair. BTS was historically performed to augment PBF but this is rarely done in the modern era. In high risk patients, PDA stenting may be used to stabilize PBF until surgical candidacy improves.
Valve sparing repair of TOF

Repair. In this operation, the PV is left in place and is plastied, usually involving surgical comissurotomies. The VSD is closed either through the TV or through an infundibular incision which is then patched closed. In some cases, there is no infundibulotomy and the RVOT muscle bundles are resected through the PV. (This may decrease the future risk of ventricular arrhythmias by preventing a transmural RV incision.) A fenestrated ASD is often left in place to permit right to left atrial flow.
Postoperative considerations. The postoperative management of TOF/PS is primarily focused upon the degree of restrictive RV physiology. A patient may be desaturated from atrial flow, which is well tolerated. Conversely, a patient without an atrial fenestration and a thickened, muscle-bound RV that receives preload poorly may be fully saturated but exhibit severe low cardiac output (poor color, feeble pulses, RA HTN, narrow pulse pressure). Vasoconstriction to maintain preload and coronary perfusion pressure, and maintenance of mechanical ventilation (if low cardiac output is present) to decrease metabolic demand may provide time for cardiac swelling to abate. RBBB is a common finding.