Overview. The Fontan procedure completes the single ventricle palliation, diverting all systemic venous return into the pulmonary circulation, further reducing the volume load on the heart to near-normal (i.e. it pumps only a single cardiac output). Typically, this procedure is performed at ~2 years of age. Life-long elevations in systemic venous pressure may contribute to hepatic cirrhosis, renal insufficiency, protein losing enteropathy, and plastic bronchitis. Exercise tolerance in adults is typically below average for age. However, Fontan survival continues to improve, and the earliest Fontan patients are now in their 40s.
Preoperative considerations. Similar to the pre-Glenn workup, a diagnostic and therapeutic cardiac catheterization is typically performed prior to a Fontan operation. As discussed on page 275, salient features of the cath include PVR, Glenn pressure, venograms (as well as coil occlusion of any VVCs, and any hint of pulmonary AVMs by contrast transit time or pulmonary venous desaturation), and aortogram (and occlusion of any APCs). The preoperative status is important, including growth and nutritional status.
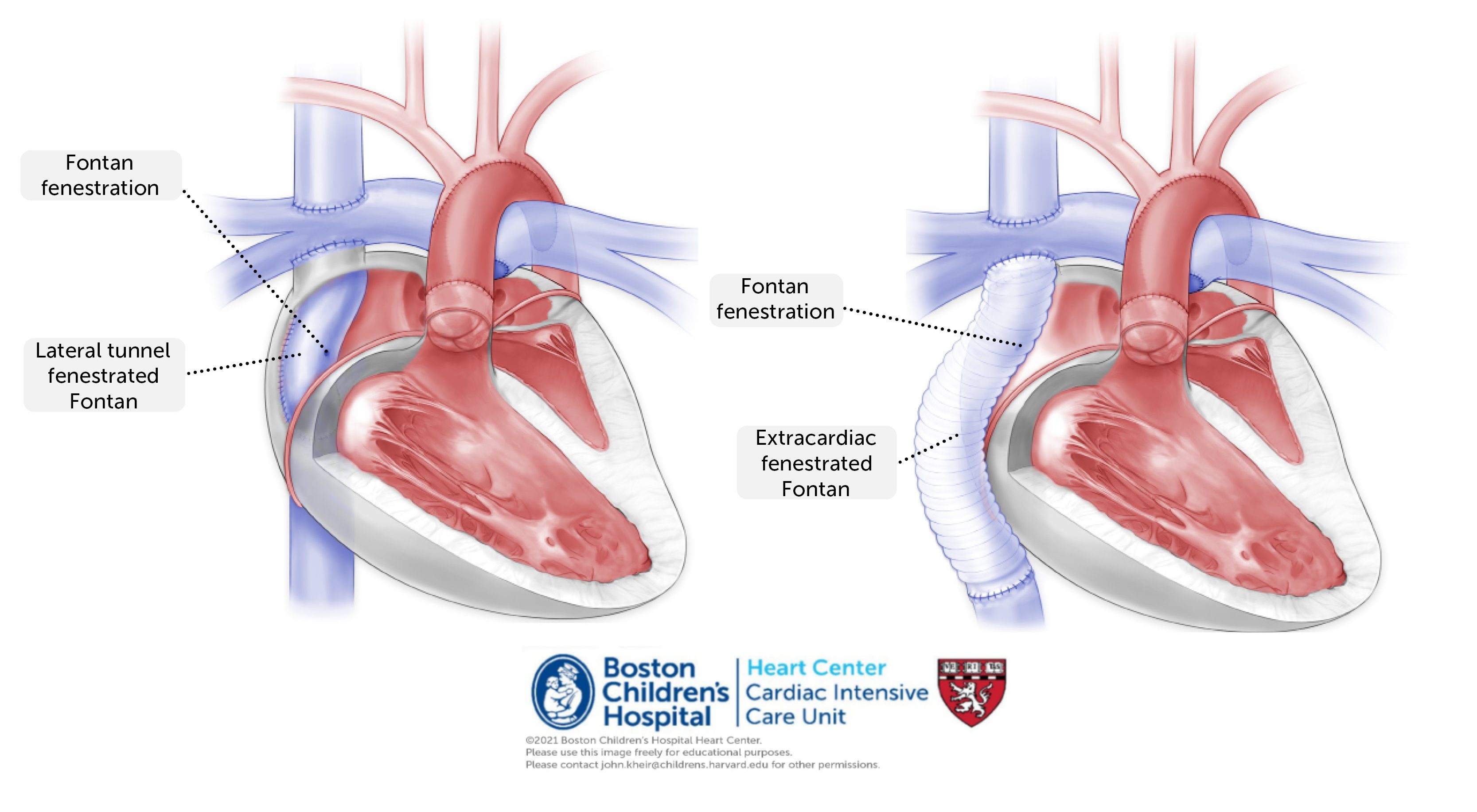
Procedure. The Fontan procedure itself includes a diversion (i.e. baffle) of IVC return to the pulmonary circulation. This can be performed via lateral tunnel, in which a patch material is fashioned into a tube-like structure that passes vertically through the lateral aspect of the atrium, or alternatively as an extracardiac conduit that abuts the atrium. A fenestration may be created (and typically is here at BCH) that allows systemic venous return to shunt from the Fontan baffle into the common atrium. This provides a ‘pop-off’ for systemic venous return to be diverted to the atrium where it can provide additional cardiac preload in settings of elevated PVR (similar in concept to a PFO). This fenestration is by necessity restrictive (typically 4 mm).
Postoperative considerations. Many patients experience an uncomplicated postoperative course following the Fontan operation, with extubation within 12-24 hours. Common considerations include:
- Assessing and maintaining fenestration patency is important. Typical saturations are in the mid-80s to mid-90s, though on 100% FiO2 the saturations may be 100% even in the setting of a patent fenestration (due to dissolved oxygen in the pulmonary veins, rendering the pulmonary vein saturation ~108% equivalent). If the lungs are open, excessive hypoxemia may indicate pulmonary AVMs or a Fontan baffle leak. Anti-platelet therapy (e.g. ASA) is typically initiated when hemostasis is achieved. Additional anticoagulation (e.g. heparin) is commonly used to diminish thrombosis in the Fontan pathway. Fenestration occlusion, particularly in the early postoperative period, may lead to hypotension (due to preload deficiency) and decreased cardiac output. When necessary, a fenestration may be created in the cath lab.
- Intermittent junctional rhythm may be present, particularly following lateral tunnel Fontan. Atrial pacing may augment cardiac output.
- Prolonged chest tube drainage (including chylous effusion) or ascites may prolong hospitalization and delay the advancement of feedings. Diuresis may diminish drainage by decreasing hydrostatic venous pressure.