Dextro-transposition of the great arteries with an intact ventricular septum
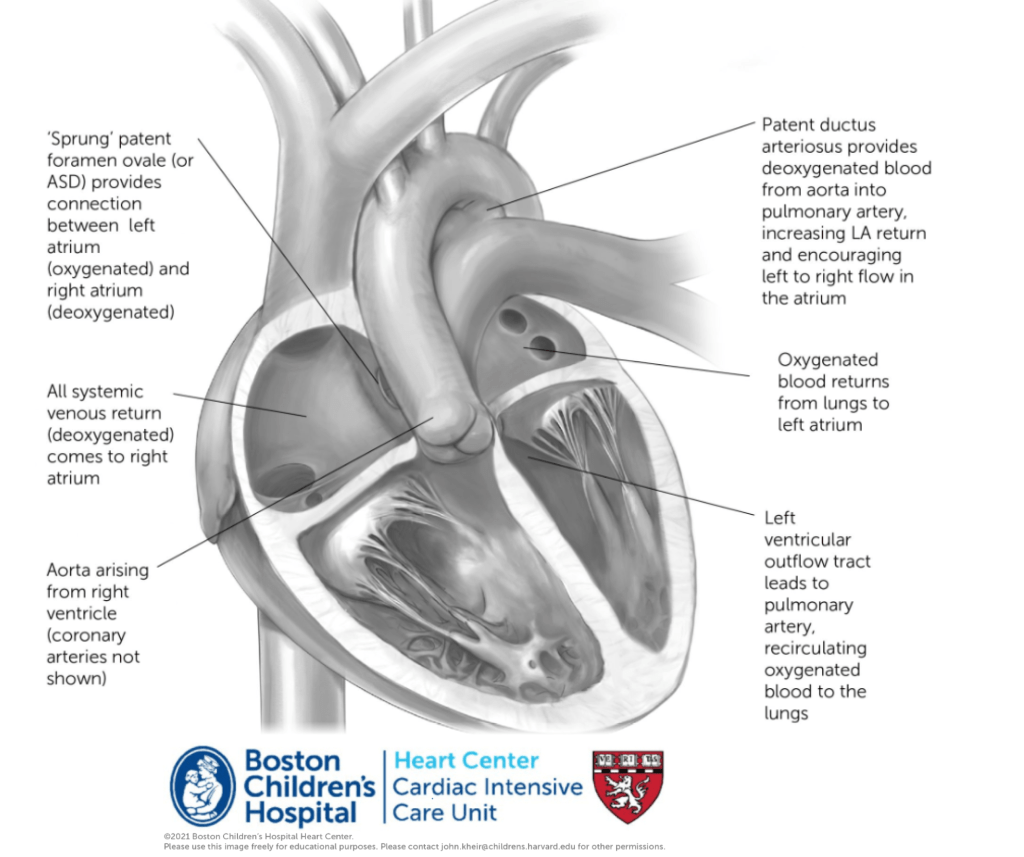
Anatomy. Transposition of the great arteries is a conotruncal abnormality in which the aorta arises exclusively from the RV and the PA exclusively from the LV. The great arteries arise from the heart in parallel and do not cross. The coronary arteries arise from the anterior and rightward aorta (associated with RV).
Physiology. When atrial situs is normal, this creates transposition physiology, in which deoxygenated blood is recirculated to the body and oxygenated blood is recirculated to the lungs. Maintenance of sufficient systemic oxygenation typically occurs by maintenance of the PDA, which increases effective (i.e. deoxygenated) pulmonary blood flow, increasing LA return and driving LA –> RA atrial flow across a PFO. Extreme hypoxemia (saturations <60%) presents an emergency. Intubation, sedation and NMB may improve hypoxemia significantly by decreasing VO2 and optimizing pulmonary vein saturations. PGE should be started in hypoxemic patients. Volume administration may stretch the PFO and improve left to right atrial shunting, improving hypoxemia. When the PFO is excessively restrictive, hypoxemia may be relieved by a balloon atrial septostomy. Additionally, because the aorta arises from the RV, intravenous catheters (particularly CVL/UVCs) should be considered LA lines and precautions should be taken to avoid introduction of air emboli.
Clinical presentation spectrum
- Unrestrictive atrial septum
- Restrictive/intact atrial septum
Preoperative considerations
Importance of feeding
Extubation?
Off PGE? Overrated…
Day of surgery related to HLOS as interesting aside?
Operative considerations



Balloon atrial septostomy
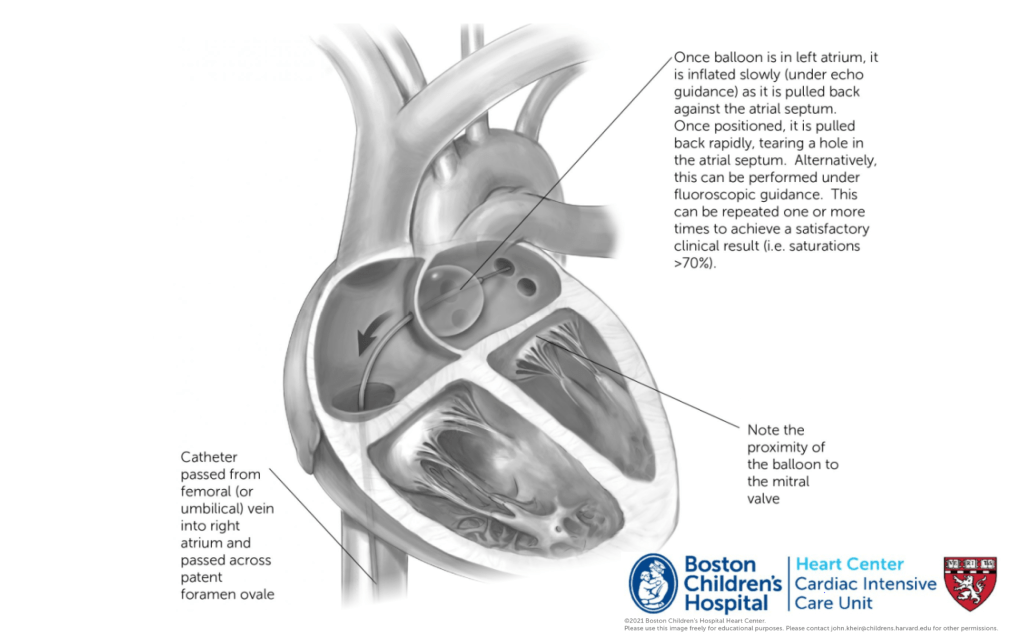
Indications. Balloon atrial septostomy (Raskind procedure; picuted above) is performed to relieve symptoms related to an excessively restrictive atrial shunt. The procedure is definitively indicated when hypoxemia is severe (e.g. SpO2<60%) despite expansion of the lungs and maintenance of the PDA. In other instances, a BAS is performed based on the echocardiographic appearance of the PFO. Even following a BAS, the atrium is almost never a common atrium, such that there is not complete atrial mixing. Instead, oxygenation still depends upon increased LA relative to RA return (i.e. atrial shunting) and the need for PGE often persists. However, if signs of LA HTN are present and surgery will be delayed, a BAS may be clinically helpful. Generally, saturations >60% are well tolerated preoperatively.
Procedural considerations. Patients may be intubated or sedated without intubation for the procedure. When planning the procedure, PRBC should be available, cath lab and echo team at bedside. Access is via femoral or umbilical vein. A catheter is passed through the PFO under echo guidance, inflated in the LA (avoiding the MV and LA appendage). Once abutting the atrial septum, the balloon is fully inflated and pulled rapidly across the atrial septum into the RA. Procedure may be repeated several times, and saturations typically improve rapidly. Complications are rare, but include injury to MV, rupture of atrial appendage, IVC or hepatic veins.
Important outcome papers
2002, Circulation – Coronary patterns and outcomes after ASO
2016, Ann Thor Surg – Outcomes in ASO with intramural coronaries
2014, JACC – Hot topics review of ASO*
2013, Circulation – Long-term outcomes following ASO – Boston
2013, Ann Thor Surg – Neoaortic root dilation following ASO
2009, Cong Heart Dis – PAB and ECMO in late presenters
2004, Circulation – Neoaortic root dilation following ASO
Technical papers
1978, Thorax – Yacoub coronary classification and transfer techniques
Historical perspectives
Although outcomes for dTGA/IVS are currently outstanding, it hasn’t always been so. Many of the operations we use for other heart diseases were first pioneered for this heart defect. Here’s a quick review.
The first approach was an atrial switch. While this relieved cyanosis, it left the right ventricle as the systemic ventricle (pumping to the aorta) for the lifetime, caused atrial arrhythmias, and other problems.
1954, Surgery – Mustard for DTGA
1978, Ann Thor Surg – Outcomes after Mustard for dTGA – Boston
The second approach was an anatomic connection between the aorta and pulmonary artery, the modern day ‘DKS’ – Damus, Kaye and Stansel all described this operation for dTGA.
The final approach was our current one, in which the great arteries are switched, including a transfer of the coronary arteries from the aortic root to the ‘neo-aortic’ root.’ Performing this operation in the newborn period was viewed with great skepticism at first, but Aldo Casteneda, John Mayer, and others at BCH proved that it could be done, and done well.